Vitamin D blood levels are inversely related to the risk of developing breast cancer. This study confirms my original work revealing that patients with the triple negative form of breast cancer (the most aggressive form) had the lowest blood vitamin D levels. See ➡︎ Triple negative breast cancer patients presenting with low serum vitamin D levels: a case series. Christa Rainville*, Yasir Khan and Glenn Tisman, M.D. Address: 10 Edelweiss, Rancho Santa Margarita, CA 92688 Cases Journal 2009, 2:8390 doi: 10.4076/1757-1626-2-8390: This article is available from: http://casesjournal.com/casesjournal/article/view/8390.
Read moreHow I Treat Multiple Myeloma Feb 2017

Above: Current treatment of multiple myeloma. (A) Newly diagnosed and (B) relapsed. *Or similar bortezomib-based triplet. **Bortezomib may be preferred for intermediate- and high-risk patients. ☨Consider salvage ASCT in patients eligible for ASCT. ➻Any of the regimenslisted for first relapse that the patient has not previously been exposed to. ASCT, autologous stem cell transplantation; DRD, daratumumab, lenalidomide, dexamethasone; DVD, daratumumab, bortezomib, dexamethasone; ERD, elotuzumab, lenalidomide, dexamethasone; IRD, ixazomib, lenalidomide, dexamethasone; KRD, carfilzomib, lenalidomide, dexamethasone; PD, pomalidomide plus dexamethasone. Rd, lenalidomide, dexamethasone; VCD, bortezomib, cyclophosphamide, dexamethasone;VRD, bortezomib, lenalidomide. dexamethasone.
Useful medications:
Therapeutic Suggestions 2016-17:
Triplet induction with VRD that combines a proteasome inhibitor and an immunomodulatory drug improves OS while ASCT improves PFS in the context of modern therapy. Posttransplant maintenance (lenalidomide in standard-risk myeloma and bortezomib in intermediate- and high-risk myeloma) improves OS.
Identification and approval of new effective drugs
• Carfilzomib (irreversible proteasome inhibitor)
• Pomalidomide (new immunomodulatory analog
of lenalidomide)
• Panobinostat (deacetylase inhibitor)
• Elotuzumab (anti-SLAMF7 monoclonal
antibody)
• Daratumumab (anti-CD38 monoclonal antibody)
• Ixazomib (oral proteasome inhibitor)
Identification of investigational drugs with
single-agent activity
• Isatuximab (anti-CD38 monoclonal antibody)
• Marizomib (proteasome inhibitor)
• Oprozomib (oral proteasome inhibitor)
• Filanesib (kinesin spindle protein inhibitor)
• Dinaciclib (cyclin-dependent kinase inhibitor)
• Venetoclax (selective BCL-2 inhibitor)
• LGH-447 (pan PIM1-3 kinase inhibitor)
• Nelfinavir (Proteasome inhibitor used in AIDS)
BCL-2, B-cell lymphoma; OS, overall survival; PFS, progression-free survival; PIM, proto-oncogene serine/threonine-protein; The surface antigen CD 319 (SLAMF7) is a marker of normal and malignant plasma cells in multiple myeloma.
Modified by Glenn Tisman, M.D.
How Is Kidney (Renal) Cancer Staged and What Is the Impact of Stage on Survival?

The Cartoon above reveals the impact of the stage (extent) of kdney (Renal cell) cancer on the approximate 5-year survival. Diagram by Glenn Tisman, M.D.
Side Effects of Newest Targeted Cancer Therapies: Is you Physician Monitoring Properly?

Often in a busy academic center or in busy physician offices routine monitoring for toxicity of the newer targeted cancer chemotherapy side effects takes a back seat. Here we empower both the physician and patient with reminders of what to look for in hope of preventing serious, sometimes life-threatening chemotherapy toxicity.
Pancreatic Cancer: Newest Adjuvant Therapies and Treatment for Advanced and Metastatic Disease

ADJUVANT: So has there been progress in therapy for pancreatic cancer? Yes and no! Appears that the best current therapy as an add on (adjuvant) to surgical removal is a combination of capecitabine (oral) and gemcitabine (intravenous).
THERAPY for METASTATIC Disease: FOLFIRINOX (a derivative of FOLFOXIRI (used initially in Italy for colorectal cancer) is the therapy with highest reported response rate however this is associated with significant side effects and requires insertion of a central venous port and use of an ambulatory infusion pump.
Elderly patients may wish to use single agent therapies such as 5-FU or gemcitabine (less effective than FOLFIRINOX.
Glenn Tisman, M.D.
Researchers Find Higher Blood Levels of Vitamin B6 Reduce the Risk for Colorectal Polyps and Colorectal Cancer by 51%.

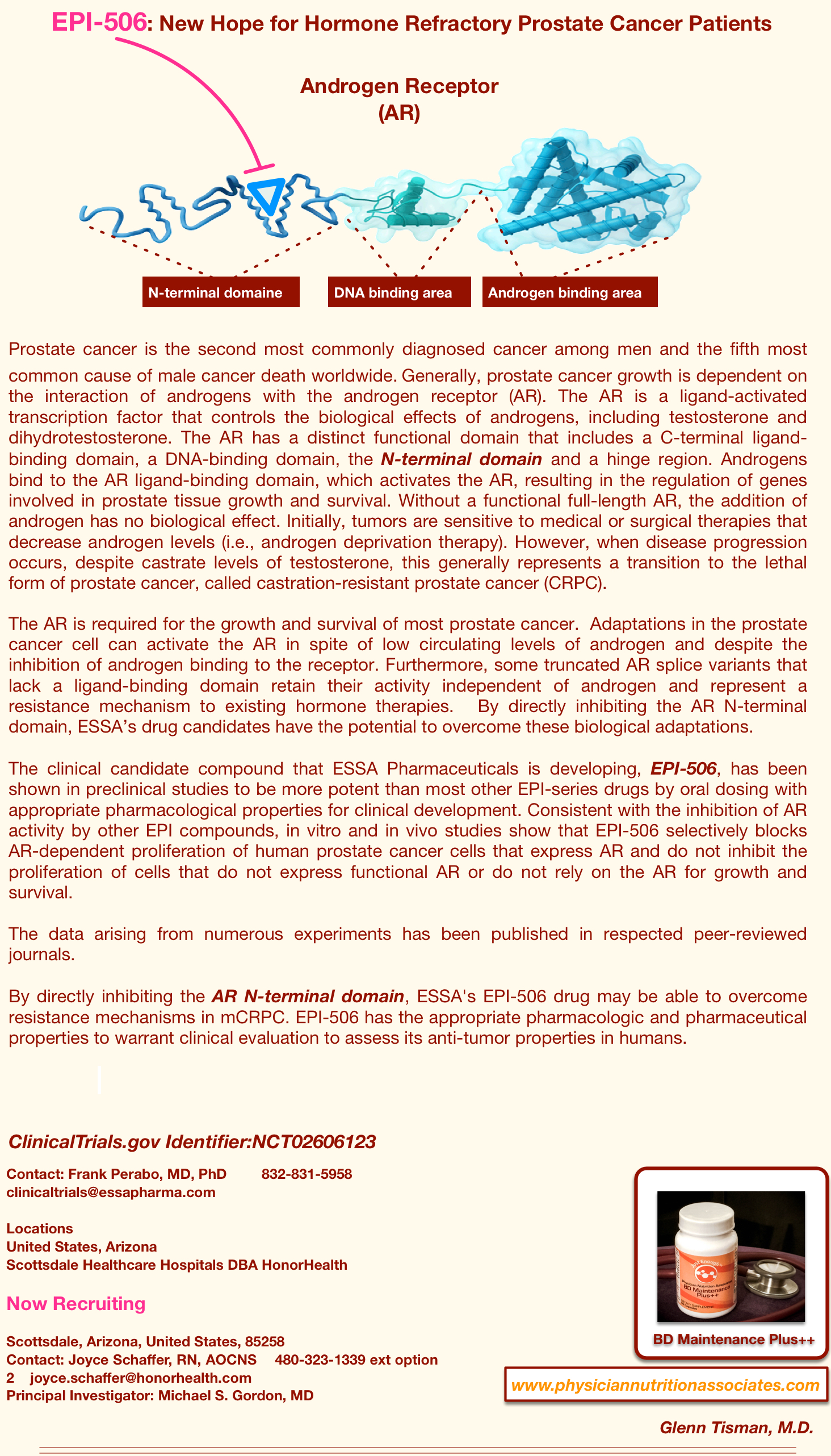
Metastatic Prostate Cancer: What we Do To The Prostate Gland May Increase Survival

There is now data from retrospective studies suggesting but not yet proving definitively that removing or radiating the remaining prostate gland may increase overall survival. An unusual approach.
Conventional medical wisdom dictated that standard therapy for patients with prostate cancer with spread from the prostate gland to a distant site such as bone should not undergo prostatectomy or radiation directed to the prostate gland but rather receive androgen deprivation therapy (ADT) aimed at tumor cells wherever they may be hiding. Why? Because in the presence of distant metastatic spread the proverbial “cat is out of the bag”. However, as we see from a new extensive retrospective evaluation of patients with metastatic disease1, surgical removal of or radiation directed to the prostate gland added to ADT in the presence of distant spread (distant metastasis (M1) of tumor was found associated with a significant increase in patient overall survival. They propose that the original source of tumor may still be exerting control of and a source for continued metastatic cell growth. There are several laboratory and a few clinical examples for such in patients undergoing surgery for several other types of malignancies i.e. renal cell cancer.
From 2004 to 2012, 6,382 men with metastatic prostate cancer (mPCa) were identified, including 538 (8.4%) receiving prostate RT. At a median follow-up of 5.1 years, the addition of prostate RT to ADT was associated with improved overall survival (OS) on univariate (P , .001) and multivariate analysis (hazard ratio, 0.624; 95% CI, 0.551 to 0.706; P , .001) adjusted for age, year, race, comorbidity score, PSA level, Gleason score, T stage, N stage, chemotherapy administration, treating facility, and insurance status. Attacking the prostate gland in the presence of distant spread (up to now a medical NO NO) revealed a superior median (55 v 37 months) and 5-year overall patient survival (49% v 33%) with prostate radiation plus androgen deprivation therapy (ADT) compared with ADT alone (P , 0.001). Landmark analyses limited to long-term survivors of ≥1, ≥3, and ≥5 years demonstrated improved OS with prostate RT in all subsets (all P , 0.05). Secondary analyses comparing the survival outcomes for patients treated with therapeutic dose radiation plus ADT versus prostatectomy plus ADT during the same time interval demonstrated no significant differences in OS, whereas both therapies were superior to ADT alone.
Is this a game changer? Possibly, however keep in mind that these results, though a product of expert statisticians, are based on a retrospective look-back. Data for this study was collected from many community hospital-based cancer registries and were provided by several American College of Surgeons-Commission on Cancer accredited facilities. Realizing that there would be an issue with data accuracy the authors of the study stated “We undertook several analytic approaches, including multivariate adjustment, propensity score matching, recursive partitioning, and landmark analyses…” sounds good but remember (junk in = junk out) regardless of the statistics.
In the Journal there is an associated editorial authored by Christopher J. Logothetis and Ana M. Aparicio from MD Anderson Cancer Center in Houston addressing the study findings. In this editorial the authors note that “controlled studies will be required to establish definitive treatment of the primary tumor as an integral part of the standard therapy of men with metastatic prostate cancer. Therefore, controlling the primary tumor should be considered only for men with metastatic prostate cancer to avoid or treatpresumably local symptoms, or as part of a clinical trial. Most importantly, the results serve as an impetus to investigate the role of the primary prostate tumor in metastatic progression and resistance to therapy”.
I personally believe that the gold standard study to confirm these initial findings of increased survival would be a contemporary prospective randomized study carried out by experienced medical research teams. However, the results of this study1 are provocative and should be kept in mind by physicians responsible for treating patients with prostate cancer as we await outcomes from current definitive confirmatory studies.
1) Improved Survival With Prostate Radiation in Addition to Androgen Deprivation Therapy for Men With Newly Diagnosed Metastatic Prostate Cancer Chad G. Rusthoven et al. JCO VOLUME 34 * NUMBER 24 * AUGUST 20, 2016. Corresponding author: Chad G. Rusthoven, MD, University of Colorado School of Medicine, 1665 N. Aurora Court, Suite 1032, Mail Stop F706, Aurora, CO
80045; e-mail: chad.rusthoven@ucdenver.edu
Glenn Tisman, M.D.